Article by Sarah Waicus (Laidlaw Scholar 2022, Medicine)
During COVID-19 many patients with suspected obstructive sleep apnoea have been reluctant to come to the hospital for overnight sleep studies with concerns about contracting or spreading the virus. This leads to my research question: can we diagnose these patients at home?
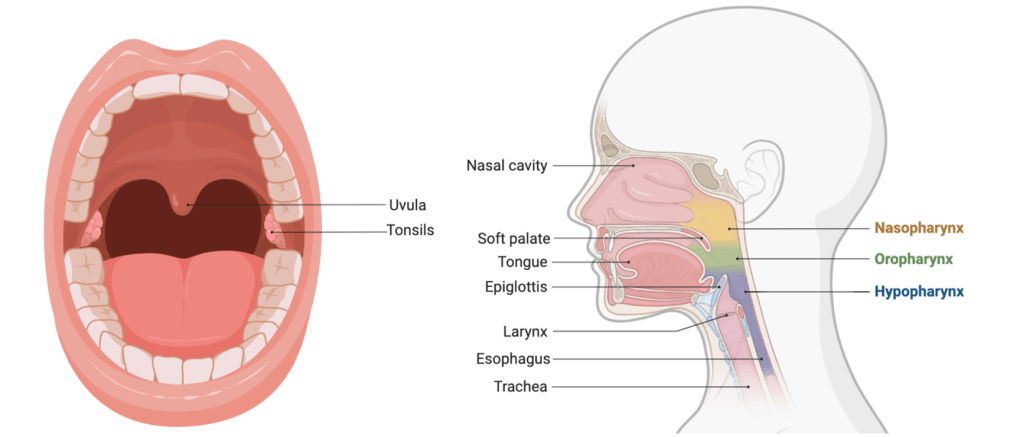
This is one account that reflects how many patients feel when suffering from sleep apnoea. Obstructive sleep apnoea occurs when the muscles in the back of your throat block breathing. These muscles include the back roof of your mouth (soft palate), uvula, tonsils, and tongue. Obstructed sleeping ultimately limits the amount of oxygen reaching your body, leading to high blood pressure, stroke, heart attack and heart failure. In addition to physical symptoms, poor sleep quality and daytime sleepiness are associated with increased road traffic accidents and mental health disorders.
Sleep apnoea is traditionally diagnosed in hospitals, where patients come for an overnight sleep study to monitor breathing, heart rate, and oxygen saturation. During COVID-19 many sleep laboratories were shut down due to patient and staff concerns about spreading the virus, as a result, many hospitals switched to at-home testing. The goal of my research was to compare the efficacy and accuracy of diagnosing sleep apnoea at home compared to in hospitals.
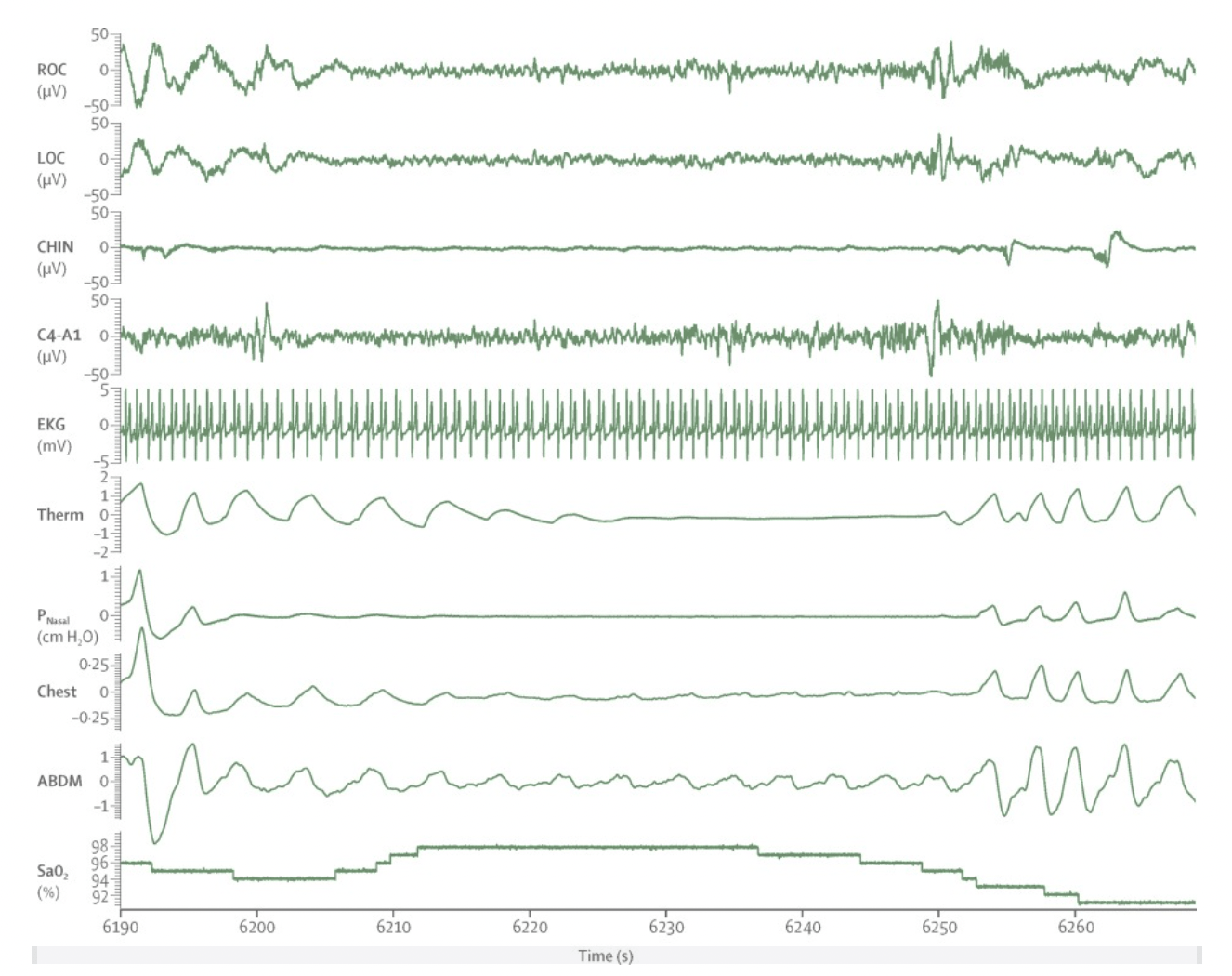
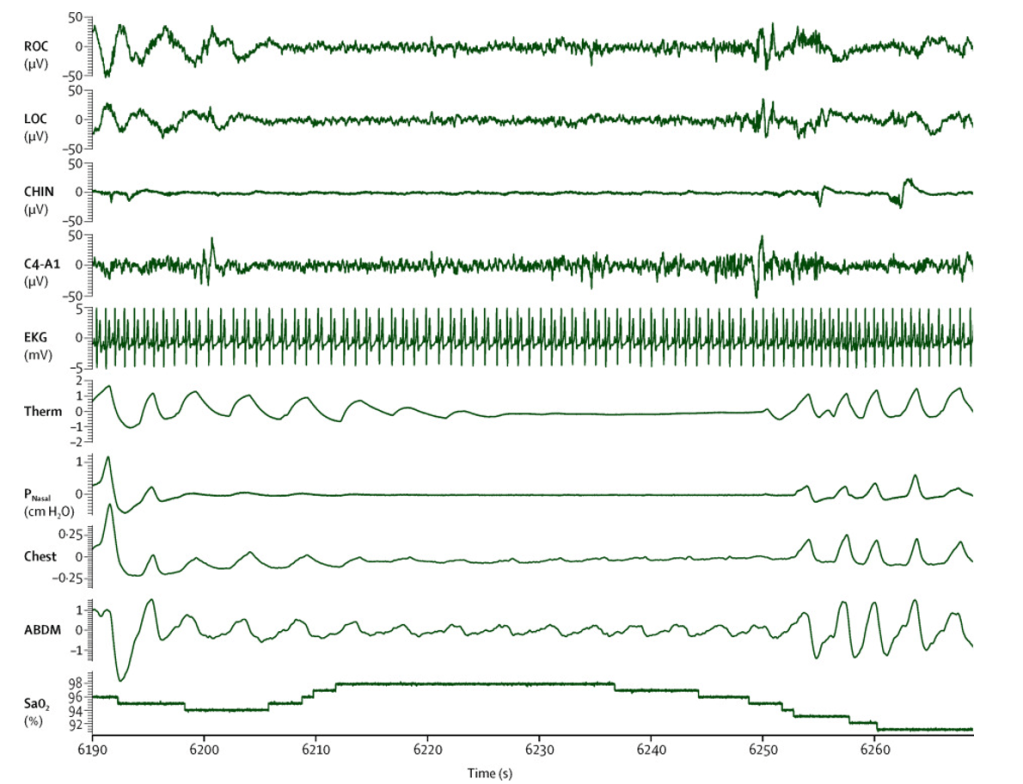
The first part of my project was data collection, taking patients’ histories and interpreting diagnostic test results that were taken at home or in the hospital. My favourite part involved interviewing and following up with patients, where I had the opportunity to listen to their life stories. The most common theme that I began to hear from patients was snoring (often from their partner) and excessive sleepiness interfering with their life. The second part of data collection was interpreting the polysomnography results. I had the privilege to learn from an experienced respiratory physician and physiologists in the hospitals who were running these diagnostic tests. These tests are incredibly difficult to run and interpret (see an example below) with much appreciation for such a hard job. For me, I was extremely lucky to have such a knowledgeable, kind team willing to help me sift through, collect, and begin to understand the data.
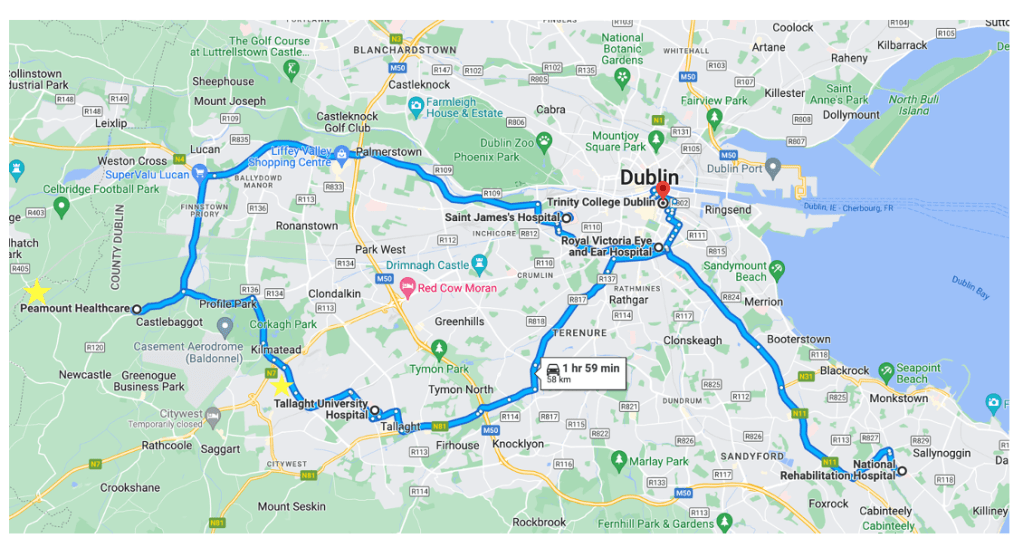
A major challenge for me during this stage was commuting between the hospitals to collect data during my medical electives. Many hours were spent on the bus going from one side of Dublin to the other in between my other hospital rotations (See map). Regardless of the commuting, I felt more connected to the community since I was physically there and could hear their stories. I would not have gotten this exposure if I was solely working virtually. Additionally, meetings at the hospitals allowed me to bounce ideas off my supervisor and see if they were feasible, because the patients, laboratory, physiologists, and data were there to help.
The second part of the project involved data interpretation. After anonymising and inputting the patient data, I had to brush up on the most difficult kind of math (in my opinion) – statistics. Trying to navigate this unfamiliar environment, I went through my notes from STATS 1 and 2 and asked for advice from a previous professor. I began to slowly analyse the data and feel like I was on the right track. This was the most difficult part of the project, as I wanted to accurately represent the data from each patient without skewing results or using the wrong test. I began to feel reassured and confident in the results after getting several rounds of feedback from my supervisor.
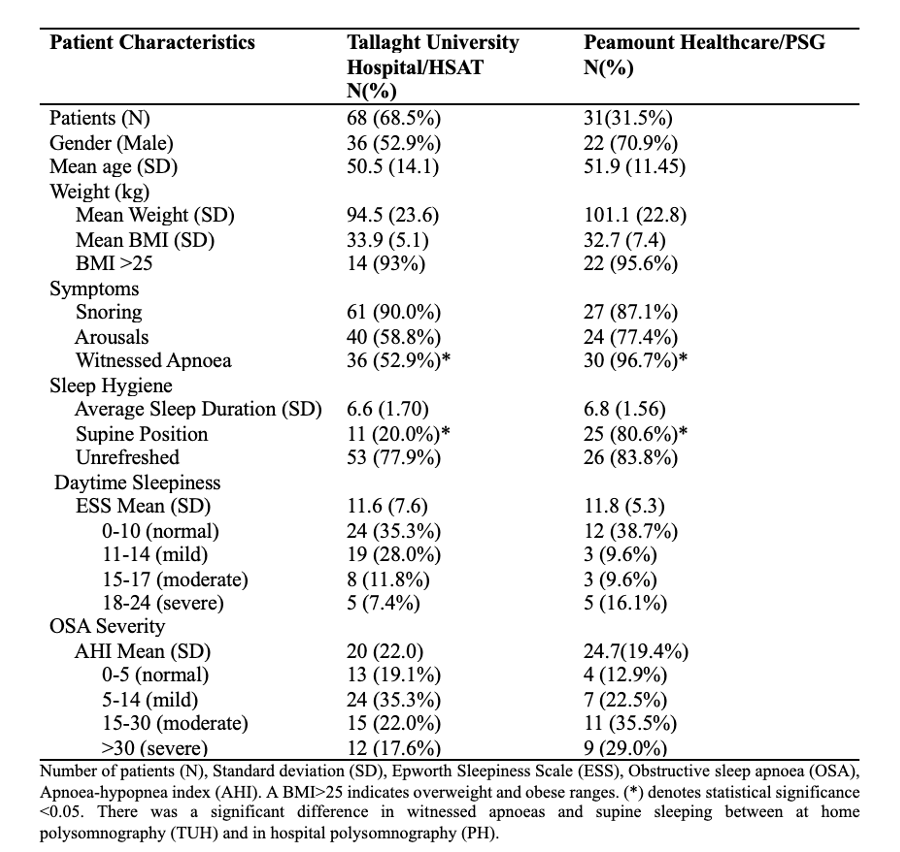
The results from the study are encouraging that home-sleep apnoea testing is similar to in-hospital testing. The only significant difference between patients being assessed at home is that there are fewer witnessed apnoeas and more supine (back) sleeping. This may be for many reasons, one of which includes the equipment in the hospital being heavier than at home and may force patients to sleep on their back during the assessment. In addition, medical comorbidities (high blood pressure, cardiac problems) and occupations (shift-workers) were expected, as many are risk factors for and are consequences of sleep apnoea.

My main takeaways from this project:
- Don’t be afraid or ashamed to ask for help from others (especially for stats).
- Taking the time to listen to patients and their stories is not only rewarding but the cornerstone of good medicine and research.
- Seeking continuous feedback to allow reflection is necessary for growth and improvement (my protocol, objectives and ideas have flourished under both scrutiny and encouragement)
I am honoured to have worked with such a great team in and outside of the hospital. I hope to continue this project as a follow-up study to assess patient experiences and treatment compliance in other hospitals in Ireland. The conclusions from this study may alleviate hospital resources and patient burden when participating in hospital sleep apnoea testing.
In the future, I hope that patients can have their whole sleep journey in terms of diagnosis, treatment, monitoring, and follow-up done entirely in their own home, without the need to visit a hospital.
